Table of Contents >> Show >> Hide
- What “home monitoring” actually means (and why the details matter)
- Why home monitoring can improve outcomes
- What the research says about outcomes: where it shinesand where it’s mixed
- Does home monitoring lower costs?
- The U.S. payment reality check (because money is a care outcome, too)
- How to make home monitoring actually improve outcomes
- A quick “who benefits most?” checklist
- Real-world experiences: what it feels like when home monitoring becomes part of life (about )
- Conclusion
Home monitoring in healthcare is basically the “receipt” your body keeps handing you. Blood pressure readings. Glucose trends. Weight changes. Oxygen levels. Symptoms. The point isn’t to turn your living room into a mini-ICU (though some of us do love a good gadget). The point is to spot problems earlier, adjust treatment faster, and avoid the expensive stufflike emergency visits and hospital stays.
One quick clarification before we go any further: this article is about health home monitoring (often called remote patient monitoring), not home security monitoring. We’re talking about your blood pressure, not your burglar. Although both can reduce stressjust in very different ways.
What “home monitoring” actually means (and why the details matter)
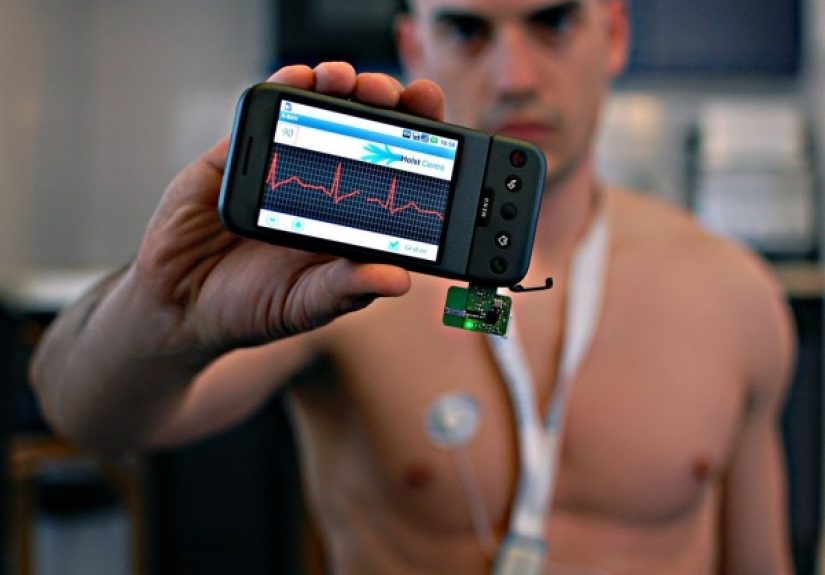
In modern care, home monitoring usually means using a device at home (like a blood pressure cuff, scale, pulse oximeter, or glucose sensor) to collect health data and share it with a care team. In many programs, the device is connected and transmits readings automatically, and clinicians use those data points to manage a conditionadjust medications, recommend next steps, or intervene before a situation escalates.
In the U.S., Medicare materials describe remote monitoring as patient-collected health data (for example, blood pressure) captured via a connected medical device that transmits data to a provider, who then uses it to treat or manage the condition. Medicare also distinguishes between remote physiologic monitoring (physiology like blood pressure or oxygen saturation) and remote therapeutic monitoring (often therapy-related data, sometimes self-reported, tied to treatment response).
That “details matter” part isn’t paperwork nitpickingit’s the difference between:
- Self-monitoring: you track readings for your own awareness, sometimes sharing them at visits.
- Remote monitoring program: readings flow to a clinical team with a plan for how to respond.
The biggest wins usually happen in the second scenariobecause data without action is just… trivia. Interesting, occasionally alarming trivia.
Why home monitoring can improve outcomes
1) It replaces “snapshots” with a movie
In-office measurements are useful, but they’re also single moments in time. Home readingswhen done correctlygive a better sense of what’s typical. That can reduce “white-coat” confusion, reveal patterns, and help clinicians make more confident treatment decisions.
2) It enables faster, smaller course corrections
Many chronic conditions don’t need dramatic interventionsthey need timely adjustments. If a care team sees blood pressure drifting upward for two weeks, they can act before it becomes a crisis. If a heart failure patient’s weight jumps quickly, that might signal fluid retention and prompt an earlier medication adjustment.
3) It boosts adherence and engagement (when designed well)
Monitoring can act like a gentle nudge: “Hey, remember this health goal we talked about?” But it only works when the program is simple, personalized, and doesn’t make patients feel like they’re being graded every morning at 7 a.m.
What the research says about outcomes: where it shinesand where it’s mixed
The honest answer to “Does home monitoring work?” is: Yes, oftenespecially for certain conditions and program designs. But it’s not magic, and not every trial shows benefits. The difference is usually the workflow: who responds, how quickly, and with what authority to change care.
High blood pressure: one of the strongest use cases
Blood pressure is an ideal target for home monitoring because it changes over time, responds to treatment adjustments, and is easy to measure (with a solid cuff and solid technique). Major cardiovascular organizations describe self-measured blood pressure monitoring at home as a validated approach for out-of-office measurement, and guidance documents note that adding remote monitoring features can further improve control compared with usual care or self-monitoring alone.
What tends to work best is not just “send numbers,” but home BP monitoring + team-based supportfor example, medication management, coaching, or pharmacist-led titration. Reviews and trials frequently show better blood pressure control when the readings are paired with real follow-up instead of disappearing into a digital void.
A practical takeaway: if you want better blood pressure outcomes, obsess less over buying the fanciest cuff and more over using it correctly. Proper positioning, resting before measurements, and consistent technique are not optional “nice-to-haves.” They’re the difference between useful data and “my cuff says I’m a hummingbird.”
Diabetes: continuous glucose monitoring is a home monitoring success story
Diabetes care has a major home-monitoring advantage: continuous glucose monitoring (CGM). CGM doesn’t just provide a single glucose valueit shows trends and time-in-range patterns that support better day-to-day decisions. The American Diabetes Association and research literature consistently associate CGM use with improved glycemic outcomes (like lower A1C) and fewer hypoglycemia episodes in many populations.
The key nuance: benefits depend on appropriate use and follow-through. A CGM sensor can provide brilliant insight, but someone still needs to interpret the patterns and decide what to changewhether that’s medication timing, insulin dosing strategy (if relevant), meal composition, or follow-up care. The “device is the hero” storyline is fun, but the real hero is the combination of data + decisions.
Heart failure and cardiopulmonary conditions: promising, but not always consistent
Heart failure is where expectations can run high (“If we monitor everything, we can prevent everything!”) and reality pushes back (“We monitored everything, and reality still happened.”).
Some forms of advanced monitoringsuch as remote hemodynamic monitoring in chronic heart failurehave reported improvements in outcomes like reductions in hospitalizations in certain studies. At the same time, not all remote monitoring strategies work. For example, randomized trials of some post-discharge remote monitoring approaches have found no improvement in outcomes like readmissions or death.
Why the mixed results? A few common reasons:
- Signal vs. noise: weight and symptoms can be important, but they can also fluctuate for reasons that aren’t clinically actionable.
- Response capacity: alerts don’t help if no one can respond quicklyor change the care plan when needed.
- Patient burden: complicated daily workflows reduce adherence over time.
- Population targeting: benefits are often larger in higher-risk patients, not necessarily across broad “one-size-fits-all” groups.
Safety and quality: monitoring can help, but it can also create new problems
Patient-safety experts often emphasize that RPM is a care model, not just a device. Data can be delayed, misread, or missed. Alerts can overwhelm staff. Patients can become anxious or fixated on normal variability. And if devices are inaccurate (or used incorrectly), programs can end up chasing phantom problems while missing real ones.
Translation: home monitoring can improve outcomesbut only when the program is designed to be safe, clinically sensible, and human-friendly.
Does home monitoring lower costs?
If you measure “cost” as healthcare spending, home monitoring can reduce costs in the scenarios where it prevents expensive events: ER visits, hospital admissions, readmissions, complications, and long lengths of stay. Systematic reviews frequently report a trend toward reduced utilization (like admissions/readmissions and length of stay) across many RPM interventionsthough results vary by condition and program design.
But “can reduce costs” doesn’t mean “always reduces costs.” Monitoring also has costs of its own:
- Devices: purchase, shipping, replacement, calibration, connectivity.
- Staffing: time to enroll patients, train them, monitor dashboards, triage alerts, and document care.
- Workflow infrastructure: software, integrations, data security, and support.
- Hidden costs: troubleshooting tech issues (aka the unofficial national pastime).
When home monitoring saves money (most often)
Programs are more likely to be cost-effective when they:
- Focus on higher-risk patients (where avoidable hospital use is more likely).
- Track a metric that is actionable (blood pressure, glucose trends, oxygen saturation in selected cases).
- Have a rapid response playbook (who calls the patient, when, and what can be changed).
- Use team-based care (nurses, pharmacists, health coachessupported by clinician oversight).
- Keep the patient workflow simple (because real life does not respect complicated onboarding manuals).
When it doesn’t save money (and may even increase utilization)
Sometimes monitoring reveals problems that were previously unnoticedleading to more visits, tests, or interventions. That isn’t automatically bad (finding unmet needs can be a win for outcomes), but it can raise short-term costs. Research on home telehealth expansion has noted scenarios where expanded monitoring may identify additional needs that increase in-person care use.
Home monitoring can also fail financially when:
- too many low-risk patients are enrolled (“We monitored everyone… including the people who were fine.”),
- alert thresholds are too sensitive (creating avoidable appointments),
- patients stop participating (so costs remain but benefits fade),
- or the program is “data collection” without “care change.”
The U.S. payment reality check (because money is a care outcome, too)
In the U.S., Medicare recognizes and reimburses certain remote monitoring services under specific rules. For example, Medicare guidance describes requirements such as an established patient relationship for remote physiologic monitoring (not necessarily for RTM), limits on who can bill, data-collection thresholds tied to code descriptors, and that only one practitioner can bill remote monitoring for a patient in a 30-day period. Medicare also notes that remote physiologic monitoring and RTM generally can’t be billed together.
Separate federal telehealth guidance also highlights requirements for RPM reimbursement (including data-collection expectations and billing limitations). Meanwhile, professional organizations have published practical billing and supervision guidance to help clinicians structure programs correctly.
Translation: the “cost difference” isn’t just about outcomesit’s also about whether the program is reimbursed and operationally sustainable.
How to make home monitoring actually improve outcomes
Pick the right goal: prevention, control, or recovery
Home monitoring works best when it has a clear goal:
- Prevention/control: tighter blood pressure or glucose control over months.
- Early warning: detecting deterioration early in high-risk patients.
- Recovery support: keeping patients on track after hospitalization or a procedure.
Each goal requires different metrics, frequency, and response workflows. If the goal is fuzzy, the results tend to be fuzzy too.
Use accurate devices and accurate technique
The simplest way to ruin a home monitoring program is to collect bad data very efficiently. For blood pressure, major heart organizations recommend an automatic, cuff-style upper arm monitor and provide guidance on how to measure correctly. Toolkits for health centers also stress using validated devices, considering cuff size (including XL cuffs), and making sure devices fit real patients (not just “average arms”).
Design for real humans (not ideal humans)
The best program is the one people can actually do when they’re tired, busy, or stressed. That means:
- short onboarding,
- clear measurement schedule,
- simple troubleshooting,
- and a clear “what happens if…” plan.
Prevent alert fatigue with tiers
Instead of treating every abnormal value like a five-alarm fire, better programs tier responses:
- Green: keep monitoring, reinforce habits.
- Yellow: recheck, assess symptoms, adjust plan if needed.
- Red: urgent outreach and clinical escalation.
This keeps clinicians from drowning in pings and keeps patients from feeling like they triggered a hospital code because they drank coffee.
A quick “who benefits most?” checklist
Home monitoring tends to deliver the biggest outcome and cost impact when at least three of these are true:
- The patient has a chronic condition where control prevents complications (hypertension, diabetes, selected cardiopulmonary conditions).
- The metric is reliable and actionable (BP, CGM trends, oxygen saturation in appropriate contexts, weight trends with a response protocol).
- A care team can respond quickly and adjust treatment.
- The patient is willing and able to participate (with support as needed).
- The program is targeted to higher-risk patients or high-utilization patterns.
If none of these are true, monitoring may still be useful for education or reassurancebut it’s less likely to move the needle on costs or outcomes.
Real-world experiences: what it feels like when home monitoring becomes part of life (about )
The first week of home monitoring often feels like a tiny lifestyle rebootpart health project, part tech support sitcom. Patients describe a “new routine” phase: finding a quiet spot, figuring out how to sit correctly, learning that talking during a blood pressure reading changes results, and realizing the dog thinks the cuff inflating is a personal betrayal. For many people, the early payoff is confidence. They start to see patterns (“My numbers are better after that morning walk,” or “That salty takeout dinner left receipts.”). When a clinician or coach responds quickly“Let’s adjust this dose,” or “Let’s repeat the readings for a few days”patients often report feeling more supported between visits, like care didn’t end when they left the clinic parking lot.
Caregivers frequently describe a different benefit: reassurance. For families supporting someone with multiple conditions, home monitoring can reduce the feeling of guessing. A trend line is emotionally easier than uncertaintyespecially when there’s a clear plan for what to do next. In some households, monitoring becomes a team sport: one person remembers the schedule, another helps record or transmit readings, and everyone agrees not to take measurements right after sprinting upstairs with laundry (because the data will absolutely tell on you).
Clinicians and nurses working with monitoring programs often report that the context is the win, not just the numbers. Instead of a single in-office blood pressure reading, they can see a week of data and make smarter decisions. With CGM, they can spot overnight patterns or post-meal spikes and tailor advice. That said, clinicians also describe the downside when programs are poorly designed: too many alerts, too little staffing, and readings arriving without the patient story behind them (“It says your oxygen droppedwere you sleeping, exercising, or accidentally sitting on the sensor?”). The most sustainable workflows filter noise, standardize triage steps, and ensure someone has the authority to act.
Patients also report a very real emotional curve. Some feel empowered; others feel watched. The line between “supported” and “surveilled” can be thin if expectations aren’t clear. People can become anxious if they interpret every fluctuation as danger. That’s why the best programs normalize variability and teach patients what matters: trends, symptom changes, and when to reach out. When done well, monitoring becomes less like “constant checking” and more like “periodic steering”a tool that helps keep health on track without hijacking the day.
Over time, successful programs often fade into the background (in a good way). The device becomes just another household itemlike the coffee maker, except it doesn’t judge you for skipping leg day. Patients still prefer fewer steps, fewer passwords, and fewer Bluetooth mysteries. But many also say that if monitoring helped prevent even one scary episode or unnecessary hospitalization, it was worth the learning curve. That’s the real litmus test: not whether the gadget is cool, but whether it meaningfully changes decisions, outcomes, and peace of mind.
Conclusion
Sodoes home monitoring make a difference in cost and outcomes? In many cases, yes, especially for hypertension and diabetes, and especially when monitoring is paired with a responsive care team that can adjust treatment quickly. Evidence is more mixed in some post-discharge and heart-failure telemonitoring approaches, which highlights a bigger truth: monitoring is not a magic wand; it’s a workflow. When the metric is actionable, the device is accurate, and the care plan is clear, home monitoring can reduce avoidable utilization, improve control of chronic disease, and support better patient experiences. When it’s “data collection without decisions,” it can add cost, noise, and frustration. The difference is design.