Table of Contents >> Show >> Hide
- What Is a Mammogram?
- Screening vs. Diagnostic Mammograms: Same Machine, Different Mission
- Types of Mammography Technology (Including 3D)
- When Should You Get a Mammogram?
- How to Prepare for a Mammogram (So the Images Aren’t Confused by Glitter… or Deodorant)
- Step-by-Step: What Happens During a Mammogram?
- Mammogram Results: Understanding BI-RADS Without Needing a Secret Decoder Ring
- Callbacks: Why Getting “Come Back for More Images” Is Often Normal
- Risks, Downsides, and Limitations (A Reality Check, Not a Scare Tactic)
- Dense Breasts: What It Means and Why You’ll Hear About It More Often Now
- Special Situations: Implants, Pregnancy, Breastfeeding, and Prior Surgery
- Cost and Access in the U.S. (So Money Isn’t the Reason You Skip It)
- FAQ: Quick Answers to Common Mammogram Questions
- Real-World Mammogram Experiences (About )
- 1) “It was my first mammogram and I was convinced the callback meant cancer.”
- 2) “Compression was annoying, but it wasn’t the medieval torture device I imagined.”
- 3) “I wore deodorant out of habit… and thought I ruined everything.”
- 4) “My report said I have dense breasts, and now I’m spiraling.”
- 5) “The best part was walking out done, not ‘thinking about it for months.’”
A mammogram is basically a low-dose X-ray that helps find breast changes earlysometimes before you or your clinician
could ever feel them. It’s also the only medical test where you briefly meet a machine that looks like a “panini press”
and thinks personal space is optional. The good news: it’s quick, it’s common, and knowing what to expect can make the
whole thing feel a lot less intimidating.
In this guide, you’ll learn what a mammogram does (and doesn’t) do, the difference between screening and diagnostic
mammograms, how to prep, what happens step-by-step, how to read results like BI-RADS, and what to do if you get called
back. We’ll also talk about dense breasts, 3D mammography, and real-world experiences people often describe after their
appointments.
Medical note: This article is general education, not personal medical advice. For recommendations tailored to your risk factors and history, talk with a qualified healthcare professional.
What Is a Mammogram?
A mammogram is an X-ray image of the breast. Mammography is designed to spot changes such as masses,
calcifications (tiny calcium deposits), or distortions in breast tissue that could signal cancer or other conditions.
Mammograms can also document “baseline” images so future exams can be compared for subtle changes over time.
Mammograms aren’t perfect (no screening test is), but they’re widely used because they can detect many breast cancers at
earlier stageswhen treatment options are often simpler and outcomes can be better.
Screening vs. Diagnostic Mammograms: Same Machine, Different Mission
Screening mammogram
A screening mammogram is the routine exam for people with no breast symptoms.
The goal is early detectionfinding something small before it causes a problem.
Diagnostic mammogram
A diagnostic mammogram is used when there’s a reason to look more closelylike a lump, nipple discharge,
skin changes, breast pain focused in one spot, or an abnormality seen on a screening mammogram. It usually includes
extra images from additional angles (so yes, it takes a bit longer).
Quick takeaway: screening is your “routine check,” diagnostic is your “zoom in and investigate” exam.
Types of Mammography Technology (Including 3D)
Most U.S. facilities use digital mammography. Many also offer 3D mammography, also called
digital breast tomosynthesis (DBT). DBT takes multiple low-dose images from different angles and
reconstructs them into thin “slices” of breast tissuekind of like flipping through pages instead of staring at a single
cover.
3D mammography can be especially helpful in certain people (including many with dense breast tissue) because overlapping
tissue on a 2D image can hide or mimic findings. Not every machine is equipped for DBT, so availability can vary by
location.
When Should You Get a Mammogram?
Mammogram timing depends on your age, personal and family history, genetics, prior radiation exposure, breast density,
and your comfort with tradeoffs like false alarms. In the U.S., you’ll also notice that respected organizations don’t
always recommend the exact same schedulebecause they weigh benefits and downsides a bit differently.
Average risk (common U.S. recommendations)
- USPSTF (U.S. Preventive Services Task Force): generally recommends screening mammography
every 2 years from ages 40 to 74 for people at average risk. - American Cancer Society (ACS): says people 40–44 can choose to start yearly screening;
45–54 should get annual mammograms; and 55+ can switch to every other year
or continue annually (as long as they’re in good health). - ACOG (American College of Obstetricians and Gynecologists): recommends beginning screening at
age 40 for average-risk individuals.
Higher risk (earlier and/or additional screening)
If you’re at higher-than-average riskfor example, you carry certain genetic mutations (like BRCA1/BRCA2),
have a strong family history, or had chest radiation at a young agescreening may start earlier and may include
breast MRI in addition to mammography. Some guidance (such as ACS) often recommends MRI plus mammogram
yearly for certain high-risk groups, typically starting around age 30.
Bottom line: if you’re unsure which category you’re in, a risk assessment conversation is worth it. It can prevent both
over-testing (extra anxiety, extra biopsies) and under-testing (missed early detection).
How to Prepare for a Mammogram (So the Images Aren’t Confused by Glitter… or Deodorant)
Preparation is simple, but a few small choices can reduce discomfort and avoid “artifact” shadows on images.
- Skip deodorant, antiperspirant, powders, and lotions on your underarms and breasts the day of your exam.
Some products can show up on imaging and create confusion. - Wear a two-piece outfit so you only need to remove your top.
- Schedule smart if you can: if your breasts are tender before your period, aim for a time when you’re less
sensitive. (Not requiredjust helpful.) - Bring prior mammogram images/reports if you’ve had exams at another facility. Comparison images can reduce
callbacks. - Tell the facility ahead of time if you’re pregnant, breastfeeding, have breast implants, or have had prior
breast surgery.
Forgot and wore deodorant anyway? Don’t panic. Many facilities can provide wipes and still do the exam.
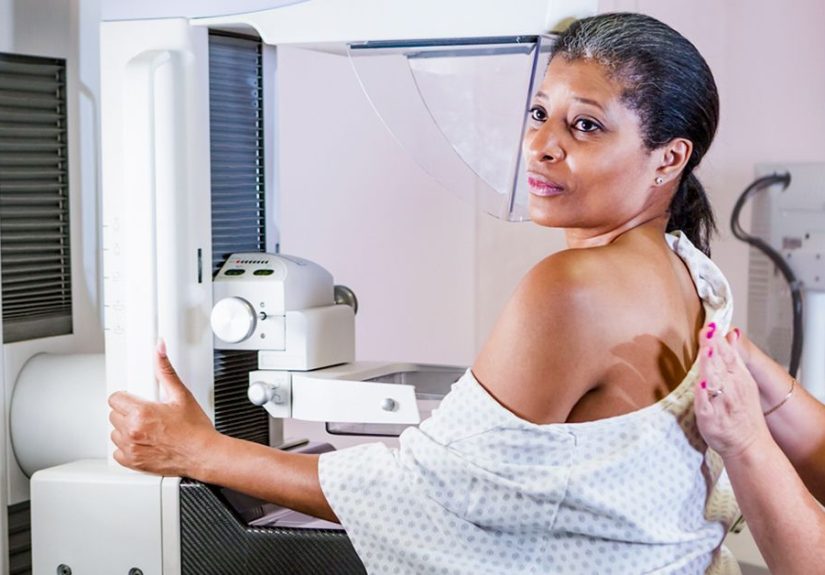
Step-by-Step: What Happens During a Mammogram?
The entire visit for a screening mammogram is often around 15–20 minutes (image time is shorter than the
total visit). Here’s how it typically goes:
- Check-in + quick questions: You may be asked about symptoms, prior breast procedures, family history, and
the date of your last mammogram. - Change into a gown: You’ll remove clothing from the waist up and take off necklaces (anything that can
sneak into the image). - Positioning: A technologist positions one breast at a time on a flat plate. Another plate comes down to
compress the breast. - Compression (the part everyone talks about): Compression spreads tissue to get a clearer image and helps
reduce motion blur. It’s firm and can be uncomfortable, but it’s briefusually only seconds per image. - Images: You’ll typically get at least two standard views per breast (more if needed). You may be asked to
hold your breath for a moment while the image is captured. - Done (and back to real life): If the images look good, you’re finished. If the technologist needs a repeat
view (positioning happens), they’ll do it right then.
Tips for comfort (without “toughing it out”)
- Say something if it’s painfultechnologists can often adjust positioning.
- Try slow breathing right before compression. Tension makes everything feel sharper.
- Let them know if you’ve had surgery or have limited shoulder mobility so they can position you safely.
Mammogram Results: Understanding BI-RADS Without Needing a Secret Decoder Ring
Many U.S. mammography centers use BI-RADS (Breast Imaging Reporting and Data System), a standardized way to
describe findings and next steps.
Common BI-RADS categories (0–6)
- BI-RADS 0: Incompletemore imaging needed (extra views and/or ultrasound). This is often a “we need a better look,” not “we found cancer.”
- BI-RADS 1: Negativeno concerning findings.
- BI-RADS 2: Benign findingsomething is present, but it’s not cancer (like a simple cyst or stable calcifications).
- BI-RADS 3: Probably benignshort-interval follow-up imaging is usually recommended (often in about 6 months).
- BI-RADS 4: Suspiciousbiopsy may be recommended to know for sure.
- BI-RADS 5: Highly suggestive of malignancybiopsy is strongly recommended.
- BI-RADS 6: Known biopsy-proven malignancyused when cancer has already been diagnosed and imaging helps guide treatment.
Important nuance: BI-RADS is about probability and next steps. It’s a map for what happens nextnot a moral judgment
on your breasts for being “complicated.”
Callbacks: Why Getting “Come Back for More Images” Is Often Normal
Being called back after a screening mammogram is common. Sometimes the radiologist simply needs a clearer view, wants to
compare with older images, or sees something that is very likely benign but worth confirming.
In the U.S., a notable portion of people are asked to return for additional imaging. This is especially common with a
first-ever mammogram, when there are no prior images to compare.
If you’re called back, ask:
Is this for extra mammogram views, ultrasound, or both? and
How soon should I schedule it?
Getting it done promptly usually shortens the anxiety window.
Risks, Downsides, and Limitations (A Reality Check, Not a Scare Tactic)
1) False positives
A mammogram can look suspicious even when no cancer is present. This may lead to extra imaging, short-interval follow-up,
or a biopsy that ends up being benign. The emotional cost is realso it’s okay to name it out loud.
2) False negatives
Some cancers are not visible on mammography, especially in dense breast tissue. That’s why it’s still important to report
new breast symptomseven if your most recent mammogram was “normal.”
3) Radiation exposure
Mammography uses a small dose of ionizing radiation. For most people, the benefit of appropriate screening
outweighs this risk. Diagnostic mammograms generally involve more images and therefore a higher dose than a screening
examstill typically considered low in medical imaging terms.
4) Overdiagnosis (the complicated one)
Screening can sometimes detect very slow-growing cancers that might never have caused problems during a person’s lifetime.
Researchers and guidelines discuss this as part of the “benefits vs. harms” balance, which is one reason recommendations
differ across organizations.
Dense Breasts: What It Means and Why You’ll Hear About It More Often Now
Breast density describes the mix of fibrous/glandular tissue and fatty tissue on a mammogram. Dense tissue
can make it harder to see cancers because both dense tissue and many tumors appear white on X-ray images (like trying to
find a polar bear in a snowstorm).
Dense breasts are also associated with a modestly higher risk of developing breast cancer. But density alone doesn’t tell
the whole storyrisk is a combination of factors.
Breast density notification (U.S. update)
U.S. mammography facilities are now required to include breast density information in reports and provide standardized
density notifications to patients under updated federal MQSA rules (enforced beginning September 10, 2024). Practically,
that means more people will see the words “dense” or “not dense” in their results and wonder what to do next.
Do dense breasts mean you automatically need extra tests?
Not automatically. The USPSTF has stated that evidence is insufficient to recommend for or against supplemental screening
with ultrasound or MRI solely based on dense breasts after a negative mammogram. However, if you have dense breasts
and other risk factors, supplemental screening (like MRI) may be appropriate.
A practical approach:
use density as a conversation starter“What’s my overall risk, and does it change my screening plan?”
Special Situations: Implants, Pregnancy, Breastfeeding, and Prior Surgery
Breast implants
You can still have mammograms with implants. The technologist may use implant-displacement views (extra images) to see
more breast tissue. Tell the facility about implants when you schedule.
Pregnancy
Routine screening is typically deferred during pregnancy for many people, but diagnostic imaging may be done if there’s a
concerning symptom. If pregnancy is possible, tell your provider and the imaging centeryour team will choose the safest
approach.
Breastfeeding
Mammograms can still be performed while breastfeeding, but breast fullness can affect comfort and images. Some people
find it helpful to feed or pump shortly before the exam (ask your clinician for personalized guidance).
Prior surgery or biopsies
Scar tissue and clips can appear on images. This is one reason prior mammograms and surgical history mattercomparison
reduces unnecessary worry.
Cost and Access in the U.S. (So Money Isn’t the Reason You Skip It)
Coverage varies, but many plans cover screening mammography, and Medicare covers screening mammograms annually for
eligible beneficiaries. If cost is a barrier, the CDC’s National Breast and Cervical Cancer Early Detection Program
(NBCCEDP) provides free or low-cost breast cancer screening to people who qualify (often based on age, income,
and insurance status).
If you’re uninsured or underinsured, it’s worth checking local programs. Many areas also have hospital financial
assistance or community screening events.
FAQ: Quick Answers to Common Mammogram Questions
Does a mammogram hurt?
Many people describe compression as uncomfortable; some describe it as painful. The intensity varies by individual
sensitivity, breast size, cycle timing, and positioning. The key is that it’s briefand you can speak up.
How soon do I get results?
Timing varies by facility and state rules. Some centers provide results quickly; others send a report within days. If you
haven’t heard back within the timeframe they gave you, call and ask.
What if I find a lump but my mammogram is normal?
Don’t ignore symptoms. A normal mammogram doesn’t automatically explain a new lump, nipple discharge, or skin change.
Your clinician may recommend a targeted ultrasound, diagnostic mammogram, or other evaluation.
Is 3D mammography always better?
Not “always,” but it can be helpfulespecially when overlapping tissue makes 2D images harder to interpret. Ask what your
facility offers and whether it’s appropriate for you.
Real-World Mammogram Experiences (About )
People rarely talk about mammograms until they’re due for oneand then suddenly everyone has a story. Here are a few
experiences that reflect what many patients commonly describe, along with practical takeaways that can make the day go
smoother.
1) “It was my first mammogram and I was convinced the callback meant cancer.”
First-timers often get called back because there’s nothing to compare the images to. One person described it as,
“They weren’t saying something was wrongthey were saying, ‘We want a clearer look.’” After a few extra views and a quick
ultrasound, the finding turned out to be a benign cyst. The takeaway: a callback is usually a request for more
information, not a diagnosis. If you do get called back, ask exactly what they’re ordering (extra views, ultrasound, or
both) and schedule it soon so you’re not stuck in the mental waiting room.
2) “Compression was annoying, but it wasn’t the medieval torture device I imagined.”
Many people psych themselves up for the painsometimes the anticipation is worse than the reality. A common description
is “strong pressure for a few seconds.” One patient said the most helpful thing they did was tell the technologist,
“I’m nervous and I tend to tense up.” The technologist coached slow breathing, adjusted the angle, and explained each step
before it happened. The takeaway: communicate. Your comfort matters, and small adjustments can make a big difference.
3) “I wore deodorant out of habit… and thought I ruined everything.”
This happens constantly. People sprint into the clinic like, “I have made an irreversible armpit mistake.” In many cases,
the staff simply provides wipes and you’re good to go. The takeaway: if you forget, tell the technologist right away.
Don’t silently worry through the whole appointment.
4) “My report said I have dense breasts, and now I’m spiraling.”
Dense breast notifications can sound scary if you’ve never heard the term. Patients often describe a mix of gratitude
(“I’m glad they told me”) and anxiety (“So… am I safe or not?”). A practical next step is to ask your clinician two
questions: (1) “What’s my overall breast cancer risk?” and (2) “Does density change my screening plan?” Some people feel
better after learning that density is one factor among many, and that the plan might still be routine mammogramspossibly
with 3Dunless other risk factors are present.
5) “The best part was walking out done, not ‘thinking about it for months.’”
A surprisingly common reflection is reliefnot because the test is fun, but because it turns vague worry into actionable
information. One person put it perfectly: “I spent more time dreading it than doing it.” The takeaway: if anxiety is
blocking you, plan a small reward afterward (coffee, a walk, a playlist on full blast). It’s not bribery. It’s
psychological first aid.